



Treatments / Main Point Of Focus

Übersicht
- Diagnostics
- Range of surgical treatments Lumbar spine
- Range of surgical treatments Cervical spine
- Range of surgical treatment Peripheral nerve compression syndromes
- Non-surgical, interventional treatments
Diagnostics
Computer tomography of the head and the entire spinal column
The Computer Tomography department on the ground floor of our clinic permits us to conduct a real-time (in emergencies even immediate) on-the-spot examination of a patient. Our computer tomography device is specially licensed for the diagnosis of disorders of the head and the entire spinal column.
Electroneurography of peripheral nerves
The motor and afferent nerve conductivity velocity (NCV) of the nerves in arms and legs is measured with the aid of electroneurography. This allows us to determine whether nerves are being restricted and compressed and whether this might lead to medical complaints.
In addition, where required, electromyographic examinations (abbreviation: EMG, the examination of electrical functions of the skeletal muscles) and somatosensory evoked potentials (abbreviation: SEP, examination of electrical signals in the brain) may be conducted.
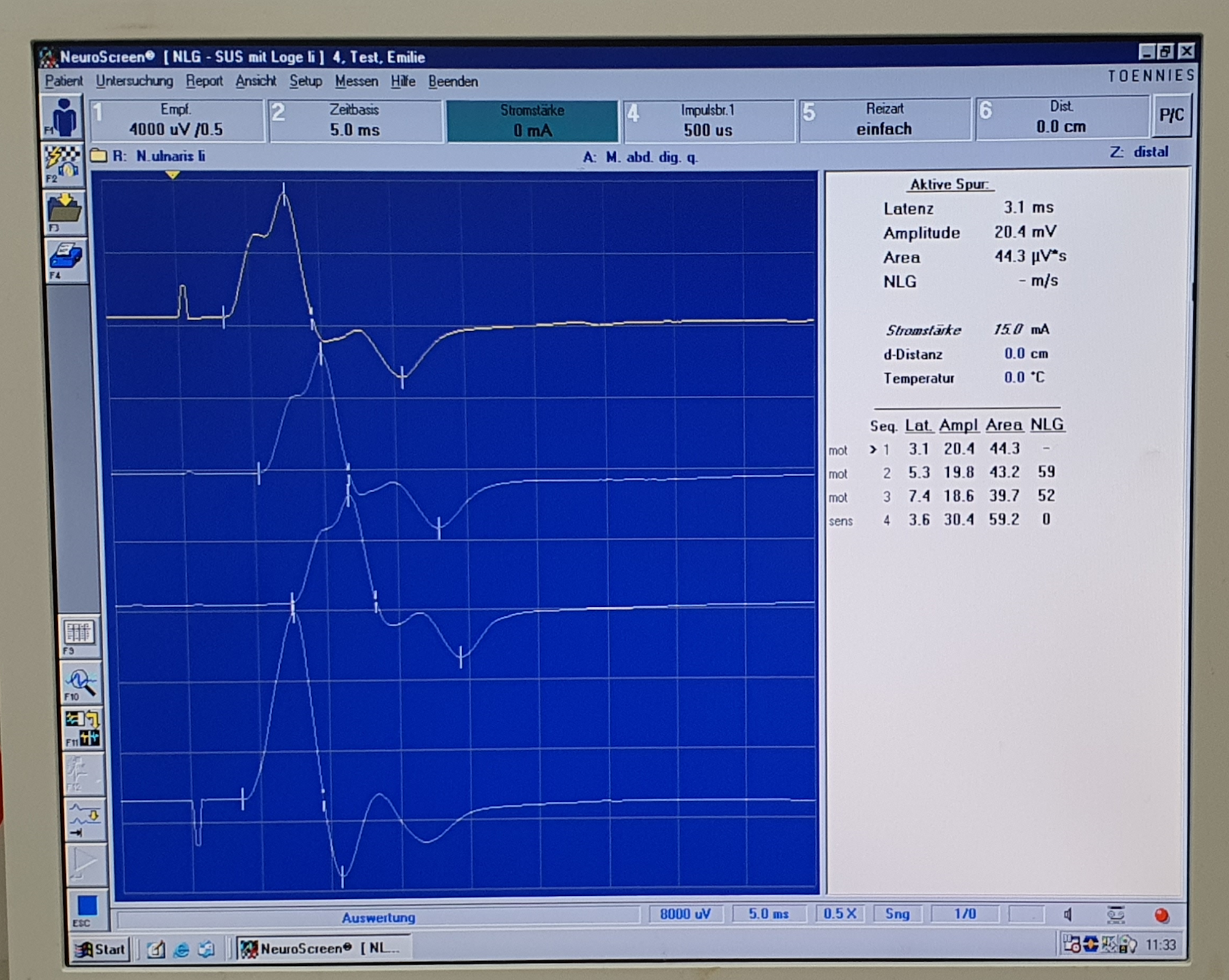
Electroneurography
Neurosonography
The ultrasound examination of the peripheral nerves (neurosonography) is a method to visualize diseases such as compression syndromes (e.g. carpal tunnel syndrome), nerve injuries, an inflammatory change or nerve tumors. It supplements the clinical examination and the electroneurography in order to select the appropriate therapy method for you.

Neurosonography
Range of surgical treatments
Lumbar spine
Microsurgical lumbar intervertebral disc operations
Lumbar (= in the area of the lower spine) intervertebral disc problems occur as a result of the degeneration of the disc nucleus which, because of its inherently poor supply situation (being fed exclusively by diffusion, no blood vessels) and man’s vertical gait, is subject to extremely high stress and heavy wear.
This disc problem leads to compression of the spinal cord and the nerve roots leaving the spine and thereby causes very severe pain that radiates to the legs and also causes motor or sensory dysfunction.
If after a thorough physical and clinical neurological examination and adequate, up-to-date imaging, an operation is necessary, this may be performed at the OstseeKlinik.
Thanks to microsurgical operating techniques, an inpatient stay after a lumbar disc operation as a rule lasts only 2 nights.

Lumbar intervertebral disc
problem, image 1

Lumbar intervertebral disc
problem, image 2
Microsurgical decompression operation for spinal canal stenosis
Lumbar spinal canal stenosis is caused by increasing arthritis of the small vertebral joints. Increasing calcareous deposits and bone accretion lead to the gradual restriction of the spinal canal.
The typical symptoms of restriction of the spinal canal are the inability to take long walks and to stand for a long time. Patients must often stop every 100 metres and sit down. Even standing up for more than a few minutes is often hardly possible.
In such a case, a decompression operation on one or more levels of the lumbar spine may become necessary.
An inpatient stay after a decompression operation in the OstseeKlinik does not last longer than three nights.
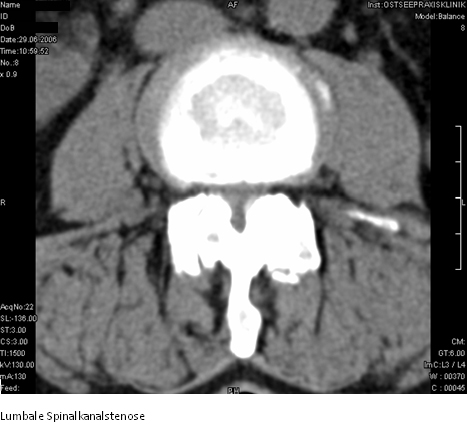
Lumbar spinal canal stenosis
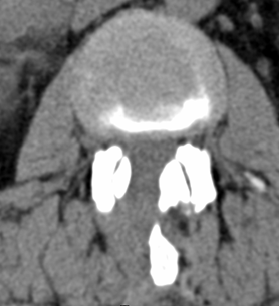
Recording postoperatively
Stabilisation operation for a slipped disc (spondylolisthesis)
Instability in the lumbar spine often appears in middle or old age as a result of increasing degenerative changes in the small vertebral joints and of increasing slackening of the ligamentous apparatus.
This instability often leads to back pain as a result of stress and is often associated with restriction of the spinal canal.
A decompression and stabilisation operation is available to treat this.
Thanks to microsurgical operating procedures, the post-operative stay after a lumbar stabilisation operation in the OstseeKlinik does not as a rule last longer than 4 nights.

Degenerative spondylolisthesis

Lumbar fusion operation
Cervical spine
Microsurgical intervertebral disc operations with ventral fusion
Disc problems also arise in the cervical spine as a result of increasing degeneration of the disc nucleus. However, static stress on the cervical spine is not so high as on the lumbar spine, so disc problems in the cervical spine are significantly rarer than in the lumbar spine.
In proven cases of disc problems with neurological dysfunction, it is often necessary to remove the problem disc, which is done via an anterior microsurgical approach.
To achieve normal stress stability of the cervical spine, an intervertebral fusion with an insert to the disc space is also required here.
The post-operative inpatient stay after a cervical disc operation lasts no longer than 2-3 nights in the OstseeKlinik.
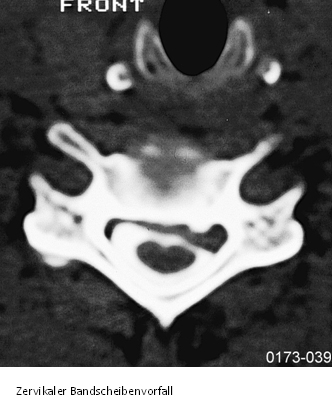
Cervical
disc problem

Cervical
stabilisation operation
Cervical disc prosthesis
With young patients with a single disc problem and only slight degenerative changes in the cervical spine, we also implant a disc prosthesis to retain freedom of movement and to prevent subsequent adjacent level degeneration.

Decompression and ventral fusion in cervical spinal canal stenosis
On the cervical spine too, bone accretion on the posterior edges of the vertebral bodies may cause considerable restriction of the spinal canal, which may lead to heavy compression of the spinal cord in the affected area.
In such a case, patients often suffer increasing insecurity when walking.
The decision on the need for an operation may only be taken after a thorough clinical neurological examination. If required, a decompression operation on the cervical spine area may then be carried out by an anterior approach, with stabilisation by ventral fusion also being required here.
The inpatient stay after this operation in the OstseeKlinik is as a rule 3 nights.

Cervical spinal
canal stenosis
Peripheral nerve compression syndromes
Decompression of the nervus medianus in carpal tunnel syndrome
Carpal tunnel syndrome is by far the most common compression syndrome of the peripheral nerves.
Many people suffer from increasing numbness of thumb, index finger and middle finger, with the complaints almost always being worst at night. Those affected wake several times a night and they have to shake and move their painful and numb hands.
Decompression of the nervus medianus in the carpal tunnel area helps. This can be done in the OstseeKlinik on an outpatient basis. These days, the affected hand no longer has to be splinted or plastered. It is bandaged, so it can be used for light tasks and heavier tasks are possible again after 6-8 weeks.
Decompression of the nervus ulnaris with sulcus nervus ulnaris syndrome
With disc problems and disc protrusions that do not lead to compression of the spinal cord and the nerve roots heavy enough to cause dysfunction (paralysis, paraesthesia), we use CT-guided periradicular therapy (PRT).
Here, with computer tomographic viewing and control, a fine needle is used directly on the affected nerve root. Then pain relief medicines are introduced. In this way the affected nerve can be treated in a targeted and controlled manner and with a truly minimal degree of invasion and rapid pain relief can be achieved.
Non-surgical, interventional treatments
CT-guided periradicular therapy, PRT
With disc problems and disc protrusions that do not lead to compression of the spinal cord and the nerve roots heavy enough to cause dysfunction (paralysis, paraesthesia), we use CT-guided periradicular therapy (PRT).
Here, with computer tomographic viewing and control, a fine needle is used directly on the affected nerve root. Then pain relief medicines are introduced. In this way the affected nerve can be treated in a targeted and controlled manner and with a truly minimal degree of invasion and rapid pain relief can be achieved.
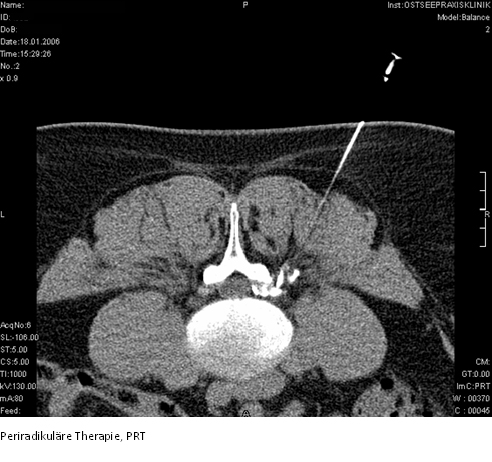
Periradicular therapy, PRT

Periradicular therapy, PRT